INCIDENCE/PREVALENCE/BURDENS ASSOCIATED WITH CARDIOVASCULAR DISEASE (CVD)
The prevention of an initial and recurrent cardiovascular event and other complications, such as diabetes and kidney failure [also known as end-stage renal disease (ESRD) or chronic kidney disease (CKD) stage 5] is an important goal in patients with a history of CVD. Each year, approximately 185,000 Americans suffer a recurrent stroke, approximately 470,000 will have a recurrent coronary attack, and an estimated 325,000 will suffer a recurrent myocardial infarction.[1] Secondary prevention strategies offer the opportunity to prevent further complications and improve outcomes by early detection and management of common comorbidities.
The burden on public health and the costs associated with chronic illnesses such as CVD, CKD, and diabetes remain high. An estimated 82.6 million American adults (1 in 3) have 1 or more types of CVD.[1] Heart failure is the fastest-growing clinical cardiac disease entity in the Unites States, affecting 2% of the population and accounting for 34% of cardiovascular-related deaths.[1] Heart failure is the most frequent cause of hospitalization in patients older than 65, with an annual incidence of 10 per 1000.[1]
An estimated 26 million people in the United States have CKD, with more than 500,000 currently being treated for kidney failure.[2] Diabetes affects 25.8 million people in the United States.[1] Unfortunately, in most cases these chronic illnesses do not occur in isolation (Figure 1).[3] CVD, CKD, and diabetes can act together as major adverse prognostic factors for morbidity and mortality[1,4,5]:
- CKD is a coronary disease risk equivalent for the development of cardiovascular events. When CVD and CKD coexist, each disease state amplifies the risk factors of the other.
- Diabetes and hypertension account for more than two-thirds of CVD risk and they are the 2 primary causes of CKD.
- Adults with diabetes have heart disease death rates about 2 to 4 times higher than adults without diabetes.
- Diabetes is the leading cause of kidney failure, accounting for 44% of new cases.
- Congestive heart failure (CHF) is the leading cardiovascular condition in CKD patients. It can interplay with hypertension and diabetes mellitus to impact CKD and vice versa.
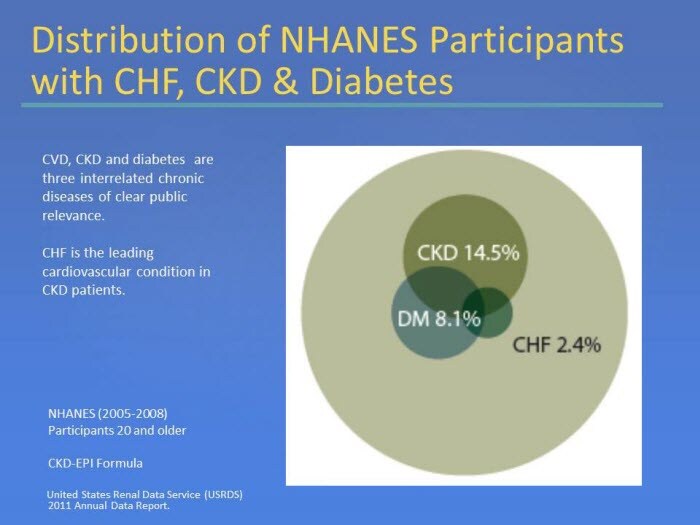
Figure 1. Distribution of NHANES Participants with CHF, CKD & Diabetes
CVD, CKD, HYPERTENSION, AND DIABETES: COMMON CONCOMITANT COMORBIDITIES THAT MULTIPLY RISK FOR POOR OUTCOMES
Two markers of kidney disease, albuminuria and reduced glomerular filtration rate (GFR), have been demonstrated to be independent risk factors for progressive kidney failure, CVD, and mortality.[6-10] CVD has numerous risk factors, including hypertension, dyslipidemia, diabetes, and CKD.[1,11] Risk factors for CVD include the "traditional" risk factors as defined in the Framingham Heart Study, as well as nontraditional risk factors specific to kidney disease (Figure 2).[11] CKD, particularly in the presence of significant albuminuria, should be considered an additional cardiovascular risk factor.[10,11]
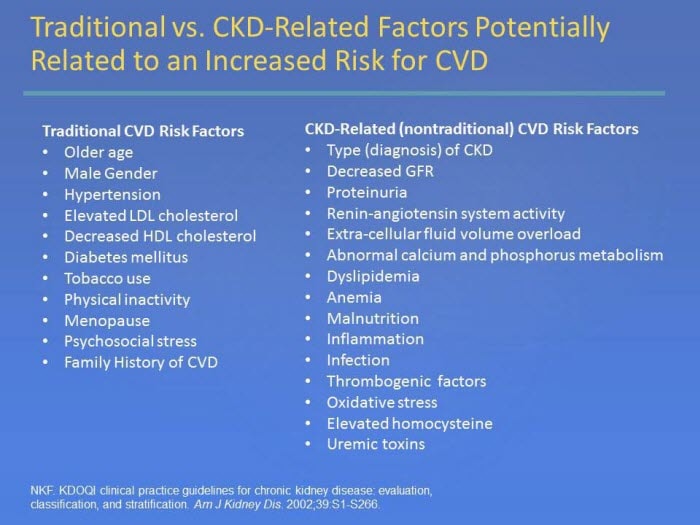
Figure 2. Traditional vs. CKD-Related Factors Potentially Related to an Increased Risk for CVD
Studies have also shown that the incidence and severity of obstructive coronary artery disease (CAD) increases as GFR declines.[12,13] CKD has also been associated with other manifestations of CVD, including ischemic heart disease, cardiac arrhythmias (most commonly atrial fibrillation), and valvular calcification.[14,15] Hypertension is present in more than 80% of those with CKD.[11]
A study by Ninomiya et al showed that high albuminuria and low eGFR are independent risk factors for cardiovascular events and mortality among patients with type 2 diabetes. The study also reveals an association with increased albuminuria and renal events (defined as death as a result of kidney disease, requirement of dialysis or transplantation, or doubling of serum creatinine to > 200 μmol/L).[9]
A collaborative meta-analysis of general population cohorts pooled standardized data for all-cause and cardiovascular mortality from studies containing at least 1000 participants and baseline information about eGFR and urine albumin concentrations. The study indicated that eGFR < 60 mL/min/1.73 m² and albumin-to-creatinine ratio (ACR) ≥ 1.1 mg/mmol (10 mg/g) are independent predictors of mortality risk in the general population (Figure 3).[7]
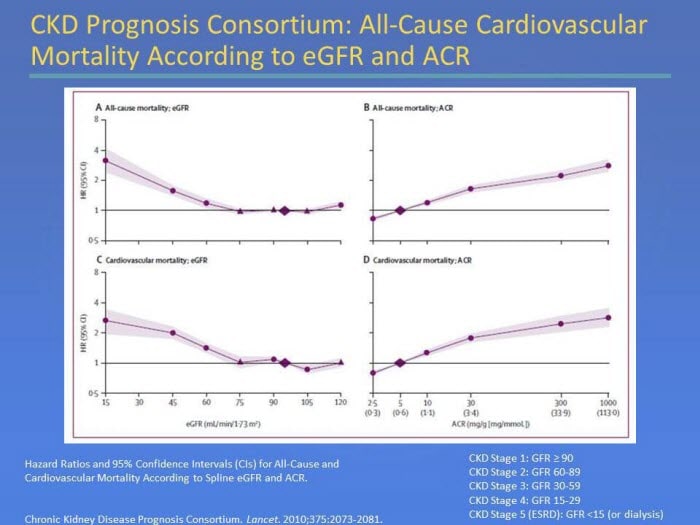
Figure 3. CKD Prognosis Consortium: All-Cause Cardiovascular Mortality According to eGFR and ACR
Kidney Disease: Improving Global Outcomes (KDIGO) initiated a meta-analysis of 45 cohorts, including 1,555,332 participants from the general population, high-risk (hypertension, diabetes, clinical cardiovascular disease), and CKD populations, which examined the relationship of eGFR and albuminuria to mortality and kidney outcomes.[8] The study found that prognosis can be assigned based on the clinical diagnosis and other key factors relevant to specific outcomes (all-cause mortality, CVD mortality, kidney failure, acute kidney injury, and kidney disease progression) (Figure 4).[8] Groups at increased risk for 1 outcome are at increased risk for all the other outcomes.
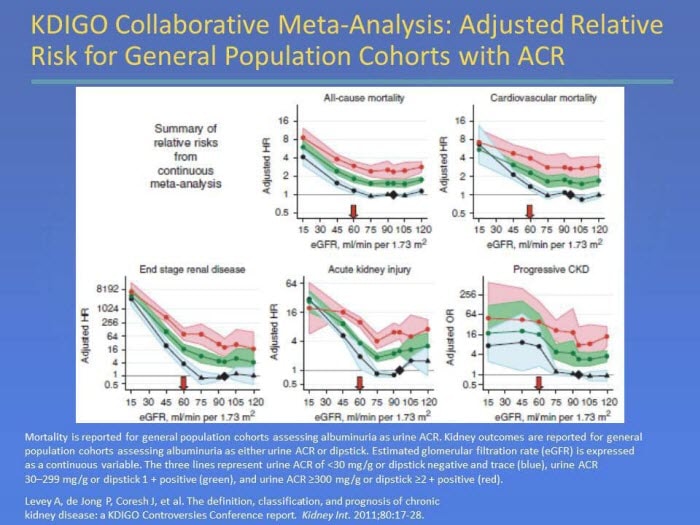
Figure 4. KDIGO Collaborative Meta-Analysis: Adjusted Relative Risk for General Population Cohorts with ACR
Within the same KDIGO study, a categorical meta-analysis (adjusted relative risk) for general population cohorts with ACR was also conducted and led to the creation of a heat map, which reflected a consensus to add albuminuria to the current CKD classification system, and to subdivide stage 3 at eGFR 45 mL/min/1.73 m2. The colors in Figure 5[8] indicate groups of patients at progressively higher risk for the major outcomes. The authors noted that clinicians, researchers, and public health agencies can use these risk categories to describe and prioritize efforts for patients and populations.[8]
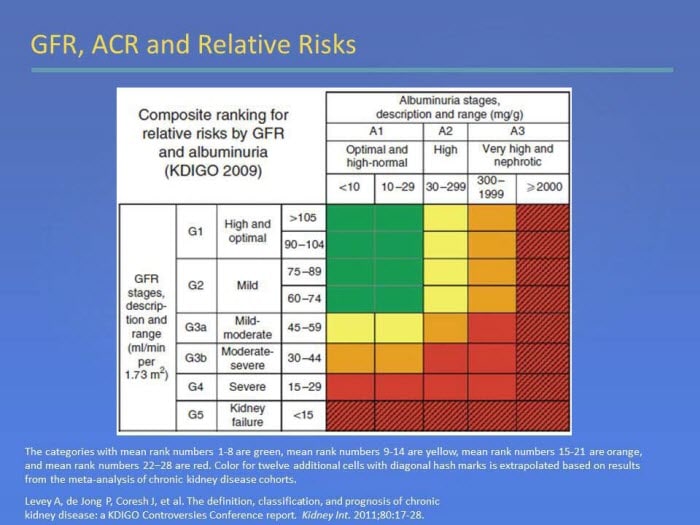
Figure 5. GFR, ACR and Relative Risks
The increasing association of CKD with CVD has given rise to a new definition of cardiorenal syndrome (CRS) and the classification of its subtypes. The term CRS is used to identify a disorder of the heart and kidneys, whereby acute or chronic dysfunction in one organ may induce acute or chronic dysfunction in the other organ. The subtypes of CRS are as follows[16]:
- Type 1 CRS: abrupt worsening of cardiac function (eg, acute cardiogenic shock or decompensated CHF) leading to acute kidney injury
- Type 2 CRS: chronic abnormalities in cardiac function (eg, CHF) causing progressive CKD
- Type 3 CRS: abrupt worsening of renal function (eg, acute kidney ischemia or glomerulonephritis) causing acute cardiac dysfunction (eg, heart failure, arrhythmia, or ischemia)
- Type 4 CRS: CKD (eg, chronic glomerular disease) contributing to decreased cardiac function, cardiac hypertrophy, and/or increased risk of adverse cardiovascular events
- Type 5 CRS: a systemic condition (eg, sepsis) causing both cardiac and renal dysfunction
Aside from the human toll, there is also a substantial cost associated with the treatment of these chronic illnesses. The total direct and indirect cost of CVD and stroke in the United States for 2008 is an estimated $298 billion.[1] Among Medicare beneficiaries alone, costs in 2009 for CKD reached $33.8 billion.[3] Total cost of diagnosed diabetes in the United States in 2007 was $174 billion. Of these, $116 billion was for direct medical costs, while $58 billion was for indirect costs (disability, work loss, premature mortality).[4] Figure 6 outlines the 2009 per person per year costs (excluding part D) for CKD, which totaled $20,432 overall, and were highest in CKD patients with both diabetes and CHF, at $34,121.[3]
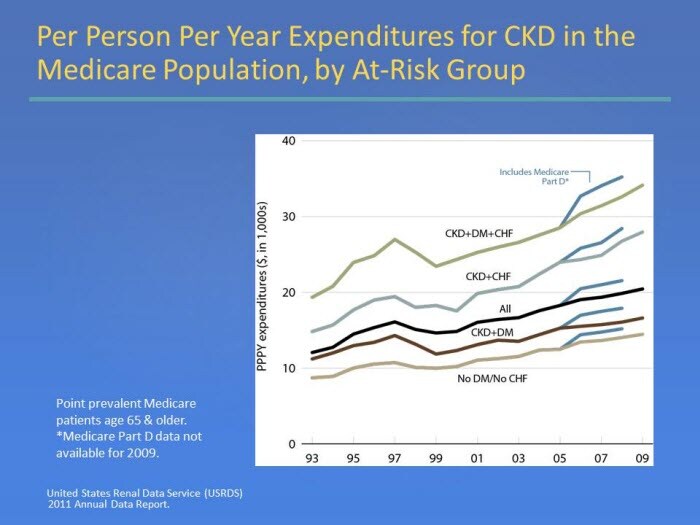
Figure 6. Per Person Per Year Expenditures for CKD in the Medicare Population, by At-Risk Group
SECONDARY PREVENTION STRATEGIES IN HIGHER-RISK PATIENTS WITH HEART DISEASE
Interventions to reduce future cardiovascular risk rely on a vigorous clinical response to risk factors and multiple comorbidities, including CKD, hypertension, dyslipidemias, and type 2 diabetes mellitus. Patient prognosis depends on early intervention, appropriate medical care, and adherence to medical plan and lifestyle changes. Successful efforts in patients with multiple risks and multiple chronic diseases require hands-on involvement that is sustained over time. The overall objective of secondary CVD prevention is to reduce the risk of a major CVD event. Given their associations and impacts, CKD should be evaluated in patients with a history of CVD.
Early Detection of CKDScreening for kidney disease consists of a serum creatinine with estimation of GFR and a spot urinary albumin-to-creatinine ratio (ACR). A 24-hour urine collection for protein is seldom needed. Moderately increased albuminuria (microalbuminuria) at any level of eGFR is considered to represent CKD.[5,11]
- Moderately increased albuminuria (microalbuminuria) is defined as an ACR of 30-300 mg/g
- Severely increased albuminuria (macroalbuminuria) is defined as an ACR > 300 mg/g
- Confirmation is required on 2 out of 3 samples over the 3-6 months following the initial detection in the absence of a urinary tract infection
The criteria for CKD include the presence of kidney damage (eg, albuminuria) or eGFR ≤ 60 mL/min/1.73 m2 for ≥ 3 months. GFR < 15 mL/min/ 1.73 m2 is defined as kidney failure. Decreased GFR can be detected by equations to estimate GFR that are based on serum creatinine, but not by serum creatinine alone (GFR calculators are available online atwww.kidney.org/GFR). GFR is the best overall index of kidney function in health and disease at this time.[11,17] Studies have documented that creatinine production varies substantially across sex, age, and ethnicity.[11,17-19] Estimates of GFR have the advantage of combining all these average effects while allowing for the marked differences in creatinine production between individuals. The level of GFR and its magnitude of change over time are vital to the detection of kidney disease, understanding its severity, and making decisions about diagnosis, prognosis, and treatment.
The stage of CKD is determined by eGFR. Once eGFR has been determined and CKD has been identified, the appropriate clinical actions can be implemented to slow the progression to kidney failure and reduce the risk of cardiovascular events. In addition to reducing CVD risk, appropriate glucose, blood pressure, and lipid control are recommended approaches to prevent or slow the progression of CKD.[5,11]Hypertension is one of the most important individual risk factors for CVD and CKD.[1,11] Therapy for hypertension typically involves pharmacological therapy and lifestyle modifications, which also includes reducing dietary sodium intake. Strategies to lower blood pressure (BP) have the potential to lower the risk of BP-related clinical complications. Treatment of hypertension can provide an opportunity to slow the progression of CKD and reduce CVD risk. Studies in the general population have shown that lowering BP is associated with a 30% to 40% reduction in risk of stroke,[23-25] and can reduce the risk of coronary heart disease (CHD) events and stroke in patients with a history of CHD or a history of stroke.[26] Studies have also indicated the benefit of lowering BP in CKD.[22,27,28]
Dietary and other therapeutic lifestyle modifications are recommended as part of a comprehensive strategy to lower BP and reduce CVD risk in CKD. The Kidney Disease Outcomes Quality Initiative (KDOQI) recommends a dietary sodium intake of less than 2.4 g/day for most adults with CKD and hypertension.[22] The American Heart Association recommends a dietary sodium intake of 1.5 g/day.[1]
The large number of drugs available can pose a challenge in knowing which drug to use for which patient. Figure 7 summarizes recommended goals for the treatment of hypertension in CVD management, in addition to specific drug class recommendations, according to indication.[21,22,29]
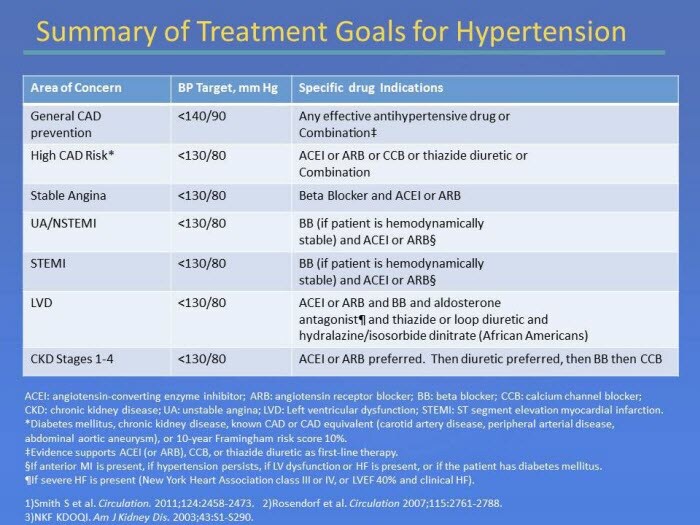
Figure 7. Summary of Treatment Goals for Hypertension
By the time individuals develop impaired kidney function, 3 or more drugs are generally needed to achieve blood pressure targets. ACE inhibitors and ARBs are preferred agents for the initial treatment of CKD.[22] Additional agents to reduce cardiovascular risk and reach target BP in the presence of CKD include diuretics (preferred), then beta blockers or calcium channel blockers.[20,22] Maximizing the dose of the first agent is recommended before adding a second agent to increase adherence and decrease side-effects. In order to minimize pill burden, and potentially adherence, combination medications can be considered once medication doses are established.
ACE inhibitors and ARBs are two classes of antihypertensive therapies that interact with the renin-angiotensin-aldosterone system (RAAS). In addition to hypertension and CVD risk reduction, RAAS blockade aims to delay the onset and progression of kidney disease. Both ACE inhibitors and ARBs are believed to reduce the glomerular permeability barrier to proteins and limit proteinuria and filtered protein-dependent inflammatory signals. Some, but not all, studies have shown that the beneficial effect of ACE inhibitors on the progression of kidney disease appears to be greater than expected due to their antiproteinuric effects.[27] In controlled trials in CKD, ACE inhibitors and ARBs have been shown to reduce protein excretion by approximately 35% to 40%. This reduction is greater than with other antihypertensive agents, even when the effect of BP reduction on urinary protein excretion has been taken into account.[27,28] Studies in normoalbuminuric normotensive patients with type 2 diabetes have not shown a benefit in reducing micoalbuminuria or cardiovascular complications among these groups.[30,31]
Several studies have shown that ACE inhibitor/ARB combinations result in modest improvement in BP and proteinuria when compared to treatment with only one of these drug classes.[32-34] This has led to the belief that a dual-agent RAAS blockade may confer cardiorenal protection. However, the renal outcomes with telmisartan, ramipril or both in people at high vascular risk (ONTARGET study) demonstrated no benefit of the ACE inhibitor/ARB combination arm vs monotherapy in either the ramipril 10 mg daily or telmisartan 80 mg daily groups on initiation of chronic dialysis.[35] In addition, RAAS blockade with the combination of an ACE inhibitor and an ARB is sometimes associated with an increase in the risk for adverse events, primarily hyperkalemia and worsening renal function, compared to either agent alone, despite a reduction in albuminuria using combination therapy.[15,20,32,36]
There can be an initial decrease of eGFR after initiation of RAAS blockade with ACE inhibitors or ARBs. This initial limited loss of eGFR is not considered a concern unless it exceeds 30%. If this level of eGFR decrease occurs, factors that predispose patients to excessive eGFR responses to RAAS blockade should be considered, including diuretic-induced hypovolemia, renal artery stenosis or NSAID use. If these conditions are not present, RAAS blockade should be continued.[20,22]
High-sodium intake further exacerbates preexisting albuminuria and increases CKD progression.[20] CHF patients with CKD often retain excessive salt and water and may require more intensive diuretic treatment than do CHF patients with normal kidney function.[15,20] ACE inhibitors and thiazide diuretics have been found to reduce stroke recurrence in patients with CKD (eGFR 30-15 mL/min/1.73 m2).[37] Most patients with CKD will eventually require a diuretic in order to achieve the BP goal since fluid retention is one of the major causes of hypertension in CKD. Generally, thiazide diuretics have been recommended in patients with GFR ≥ 30 mL/min/1.73 m2, while loop diuretics have been recommended in patients with GFR < 30 mL/min/1.73 m2.[22] However, the choice of diuretic (thiazide or other) may depend on multiple factors (eg, GFR level, extracellular fluid volume, adverse effects), and initial low doses and slow upwards titrations should be considered. Aldosterone receptor antagonists have been identified as a treatment for CHF, in particular advanced heart failure with significant potassium losses. They are also used as adjunctive therapy for resistant hypertension. The concern about these agents is the risk for hyperkalemia. Studies show that the highest risk is among patients already on diuretics with RAAS and who have a GFR < 45 mL/min/1.73 m2 and serum potassium > 4.5 mEq/L.[20,38,39]
Beta blockers are generally recommended for secondary prevention following a myocardial infarction in patients without CKD.[21] They also have an important role in patients with CHF, angina, and ischemic heart disease, and are generally considered to be neutral to kidney function.[15,22,40] However, certain beta blockers may be contraindicated in CKD due to renal excretion routes (eg, atenolol, nadolol or sotalol).[41] They are also generally not advised until hemodynamic stabilization has occurred. Recent data on bisoprolol or carvedilol supports the use of beta blockers in CKD patients with chronic heart failure.[42,43] Therefore, the use of beta blockers can be beneficial in certain cases. Their administration can be slow, careful and titrated, and given during the more stable phase of cardiac failure.[40]
Management of Dyslipidemias in CKD: Use of Lipid-Lowering AgentsThe relationship between dyslipidemias and CVD in the general population is comprehensive.[1,23,44,45] High cholesterol has become known as one of the major controllable risk factors for CHD, heart attack, and stroke. Many factors can influence the occurrence of dyslipidemias, including diet, lifestyle choices, other medical conditions, and certain medications. Along with CVD, dyslipidemias are associated with decreased kidney function.[46] Therefore, it is prudent to evaluate dyslipidemias in patients with CKD to detect abnormalities that may be treated to reduce the risk of CVD.
Studies have shown that low-density lipoprotein cholesterol (LDL-C) is a predictor of individual CHD risk and stroke.[1,25,44]Therefore, lowering LDL-C is the primary focus for the management of dyslipidemia, by lifestyle interventions and, usually, pharmacotherapy to achieve recommended goals. Guidelines recommend lipid-lowering medication when lifestyle modifications are insufficient to lower LDL-C, and when patients have established CVD (secondary prevention).[23,44] Primary and secondary prevention studies in patients without CKD have shown the benefit of therapeutic interventions to lower LDL-C to target values.[23,47-54] Studies have also shown that the greater the reduction in LDL-C, the greater the reduction in stroke risk in non-CKD patients.[23,55]
The general approach to treating dyslipidemia in adults with CKD follows the approach adopted by the ATP III.[44,46] Figure 8[44,45] summarizes the definition of dyslipidemias as defined in the ATP III guidelines. The ATP III guidelines are currently being updated (ATP IV). Modifications to LDL-C goals since the original publication include recommendations that LDL-C should be < 100 mg/dL for all patients with CHD and other clinical forms of atherosclerotic disease, and that it is also reasonable to treat to LDL-C < 70 mg/dL in patients at highest risk. These changes defined optional lower target cholesterol levels for very high-risk CHD patients, especially those with acute coronary syndromes. When the < 70 mg/dL target is chosen, it is generally recommended to increase statin therapy in a graded fashion to determine a patient’s response and tolerance.[44,45]
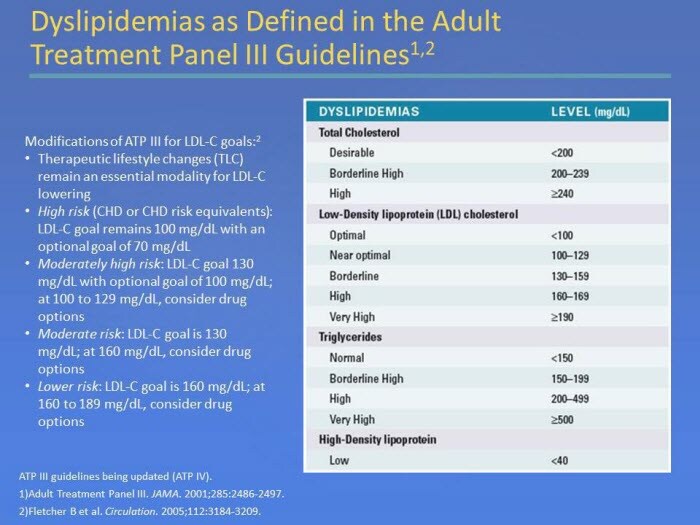
Figure 8. Dyslipidemias as Defined in the Adult Treatment Panel III Guidelines
Because of the high rate of CVD in patients with CKD and the overall safety of most medical therapies for dyslipidemia guidelines, KDOQI guidelines recommend pharmacological therapy of dyslipidemia in CKD stages 1-4 (eGFR 90-15 mL/min/1.73 m2), if therapeutic lifestyle changes alone are insufficient, and there is no evidence of acute or chronic liver disease.[45,46] Statins have been shown to be effective in lowering LDL-C in patients with CKD stages 1–4 (eGFR 90-15 mL/min/1.73 m2), and could reduce cardiovascular events. Patients with CKD often require treatment with a combination of lipid-lowering drugs, because they have abnormal levels across multiple lipid categories (Figure 9).[5,46]
Patients with CKD should be monitored for signs and symptoms of myopathy. The risk of myopathy from statins is increased by CKD, advanced age, small body frame, and concomitant medications (eg, fibrates, nicotinic acid, cyclosporine, azole antifungals, macrolide antibiotics, protease inhibitors, nefazodone, nondihydropyridine calcium antagonists, and amiodarone).[46] Higher doses of lipid-lowering medicines have also been associated with increased risk of myopathy, including patients with reduced kidney function.[56,57] Therefore, doses of some lipid-lowering medicines may need to be modified in patients with advanced CKD.
The FDA recently issued revised safety label changes to statin drugs. The labels now recommend that liver enzyme tests should be performed before starting statin therapy and as clinically indicated thereafter, as opposed to routine periodic monitoring. The label revisions also include information about the potential for generally nonserious and reversible cognitive side effects and reports of increased blood sugar and glycosylated hemoglobin (HbA1c). However, the FDA continues to believe that the cardiovascular benefits of statins outweigh these small increased risks.[58]
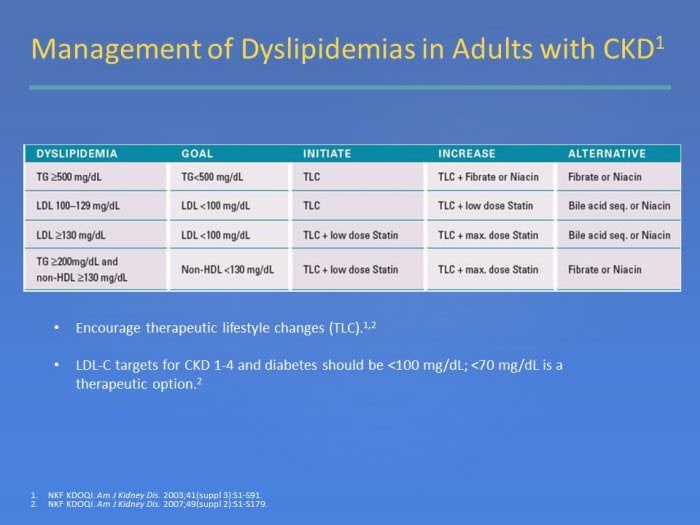
Figure 9. Management of Dyslipidemias in Adults with CKD1
A post-hoc analysis of data from the Pravastatin Pooling Project (PPP), a subject-level database combining results from three randomized trials of pravastatin, showed that pravastatin reduces the rates of cardiovascular events and all-cause mortality in people with, or at risk for, coronary disease and simultaneous mild or moderate impairment of kidney function.[59]
A subanalysis of the TNT (Treating to New Targets) study investigated the effects of intensive lipid lowering with atorvastatin in patients with CHD, with and without preexisting CKD. The results of this study support the use of high-dose statin therapy (80 mg atorvastatin) to lower target LDL-C levels for prevention of cardiovascular events in high-risk patients with mild-to-moderate CKD and CHD.[60]
A post-hoc subgroup analysis of data from the CARE (Cholesterol and Recurrent Events) study suggested that pravastatin is effective and appears safe for secondary prevention of cardiovascular events in persons with mild CKD. Statins may be underused in this setting, so the authors suggested that if these drugs were more widely used, this strategy might safely reduce the burden of cardiovascular disease in this population.[61]
The Study of Heart and Renal Protection (SHARP) trial studied the effects of lowering LDL-C in patients with CKD, but with no known history of myocardial infarction or coronary revascularization. The study showed that reduction of LCL-C with simvastatin 20 mg plus ezetimibe 10 mg daily safely reduced the incidence of major atherosclerotic events by 17% in patients with CKD.[62]
Although statins have shown benefits in lowering LDL-C and reducing CVD events in patients with mild-to-moderate CKD, the beneficial evidence on the use of statins in dialysis patients has been less certain. Two large trials (4D [Deutsche Diabetes Dialyse Studie] and AURORA [Use of Rosuvastatin in Subjects on Regular Hemodialysis: An Assessment of Survival and Cardiovascular Events]) comparing statins with placebo in hemodialysis patients did not demonstrate benefits.[63,64]
Patients on dialysis did not show a statistically significant reduction in risk of the primary outcome in the SHARP trial. The SHARP investigators concluded that this group may still be likely to benefit because of lack of statistical heterogeneity. They noted that the trial was not expected to have sufficient statistical power to allow reliable estimation of effects on major atherosclerotic events in particular clinical circumstances, so subgroup analyses were planned only as tertiary assessments.[62]
The lack of a reported benefit of statin therapy among dialysis patients is in contrast to other studies in patients with earlier stages of CKD, which showed a benefit. More studies are needed to demonstrate whether the benefits shown in earlier stages of CKD may or may not continue through CKD stage 5.
Patients who develop minor adverse effects from a statin may be able to tolerate a reduced dose or a different statin. However, for patients who do not tolerate a reduced dose or another statin, a second-line agent can be used. Either a bile acid sequestrant or nicotinic acid can be used to effectively reduce LDL-C. Treatment with a fibrate or nicotinic acid should be considered if therapeutic lifestyle changes (TLC) are not sufficient to reduce triglycerides to < 500 mg/dL.[46] Nicotinic acid (niacin) is considered effective in increasing HDL cholesterol levels (a 15% to 35% increase) in the general population, has beneficial effects on triglyceride levels (a 20% to 50% reduction), and has less significant but favorable LDL-C lowering effects (5% to 25% reduction).[46]
Evidence from studies in the general population indicates that bile acid sequestrants are generally safe and effective in lowering LDL-C by 15% to 30%. Bile acid sequestrants currently are recommended as second-line agents for reducing elevated LDL-C levels in patients with CKD.[46] Bile acid sequestrants may increase triglycerides in some patients and are contraindicated in patients with elevated triglycerides (≥ 400 mg/dL). For patients who continue to have LDL levels ≥ 100 mg/dL despite TLC and optimal treatment with a statin, consideration should be given to adding a bile acid sequestrant, if triglycerides are < 400 mg/dL.[46]
Fibric acid derivatives (fibrates) are indicated when hypertriglyceridemia (serum triglycerides ≥ 500 mg/dL) is the primary lipid abnormality. They have been shown to reduce triglyceride levels by up to 30% to 50%. However, fibric acid derivatives are excreted by the kidney and may cause myositis, particularly when used in conjunction with statins.[46] A characteristic of this class of drugs is their tendency to cause a moderate reversible increase in serum creatinine, as reported by the FIELD (Fenofibrate Intervention and Event Lowering in Diabetes) study.[65] In general, fibric acid derivatives are better tolerated than nicotinic acid. The benefits of drug therapy for hypertriglyceridemia should be weighed against the risks. The risk of complications (particularly myositis and rhabdomyolysis) is increased in CKD patients.[66]
Antiplatelet Therapy in CKDAntiplatelet therapy is another important component for secondary prevention of CVD, along with BP control, lipid management, and lifestyle modification. Studies have demonstrated the benefit of antiplatelet therapy in CVD patients without CKD.[21,23,67] However, patients with CKD pose a special challenge in the case of antiplatelet therapy. Stroke risk increases with declining kidney function.[68] Patients with CKD are also at higher risk for coronary syndrome.[15] However, antiplatelet agents carry the risk of bleeding, which is of particular concern in the case of CKD because these patients have inherently higher risks of bleeding associated with their disease. In addition, heparin is routinely used with hemodialysis.[15,69]
The use of aspirin in patients with CKD has indicated benefits. Exploratory analyses of randomized trials show that low-dose aspirin for primary prevention of stroke in hypertensive patients with CKD stages 3-4 (eGFR 59-15 mL/min/m2) and antiplatelet therapy for prevention of major vascular events are effective in patients receiving hemodialysis.[15,70] A prospective coronary care unit registry of patients with ST-segment elevation myocardial infarction showed that aspirin reduced in-hospital mortality by 64.3% to 80% across all quartiles of creatinine clearance (CrCl).[71,72] The UK HARP (Heart and Renal Protection)-1 trial and the DOPPS (Dialysis Outcomes and Prescription Patterns Study) showed that low-dose aspirin in CKD patients was not associated with increased major bleeding or progression of CKD.[71,73,74] As with all patients, aspirin allergies (eg, hives, irritated skin, swelling of the lips, tongue or face), intolerance (eg, gastrointestinal bleeding), and other contraindications should be monitored and documented.
Studies on treatment approaches using aspirin/clopidogrel in conjunction with beta blockers and ACE inhibitors/ARBs appear to have similar benefits in CKD and non-CKD patients with acute myocardial infarction.[15,75,76]
A meta-analysis found that antiplatelet regimens in persons with CKD who have or are at risk for CVD reduce fatal or nonfatal myocardial infarction by approximately 33%, but have uncertain effects on stroke or all-cause and cardiovascular mortality.[77]
Research on the use of antiplatelet agents in CKD is ongoing. When using antiplatelet agents in patients with CKD, the goals of CVD prevention need to be weighed against the risk of bleeding.
Type 2 Diabetes Management and Antihyperglycemic Agents in CKDType 2 diabetes mellitus is frequently found in patients with CVD and CKD, and can compound the risk of long-term complications in these patients. Like CVD and CKD, diabetes is a complex chronic disease that typically involves multiple intervention strategies, which not only include glycemic control, but also lifestyle modifications (low-sugar diet and physical activity) and control of BP and lipids.[5,21,80] In addition to diet and medication to lower blood glucose levels, patient education and self-care practices are also important aspects of disease management. Many people with type 2 diabetes can control their blood glucose by following a healthy meal plan and exercise program, losing excess weight, and taking oral medication. Medications for each individual with diabetes will often change during the course of the disease. Some people with type 2 diabetes may also need insulin to control their blood glucose.
Hyperglycemia is the defining feature of diabetes, and glycemic control is a crucial part of diabetes management. Intensive glycemic control has been shown to reduce microvascular complications (retinopathy, nephropathy, and neuropathy). Studies have also indicated a relationship between HbA1c and CVD.[80-82] Hyperglycemia is an important risk factor for both diabetic nephropathy with albuminuria and retinopathy, as well as less specific forms of CKD. HbA1c has been associated with the development of CKD, independent of traditional risk factors. The strong significance of HbA1c in its association with the presence of CKD occurred even in the absence of albuminuria and retinopathy in the Atherosclerosis Risk in Communities (ARIC) Study.[83] In this study, individuals without diagnosed diabetes at baseline were followed for 14 years. Even in the absence of diagnosed diabetes over that time period, higher levels of HbA1c were associated with the development of CKD.[84]
People with CVD, CKD, and/or type 2 diabetes do not represent a uniform population, so individual circumstances must be incorporated into therapeutic targets. The therapeutic goal should be based on potential patient risk and benefits. Patients with CKD and diabetes with insufficient glycemic and BP control are at a high risk for developing both CVD and progression of nephropathy. The risk of hypoglycemia is increased in patients with substantial decreases in eGFR (CKD stages 4 and 5) for 2 reasons: (1) decreased clearance of insulin and of some of the oral agents used to treat diabetes and (2) impaired renal gluconeogenesis with reduced kidney mass.[85] Therefore, determining the safe and appropriate level of glycemic control is complex when CKD, diabetes and CVD are all present.
Diabetes treatment regimens may need to be modified in the presence of CKD. Reduced GFR often mandates a decrease in the dosage of these drugs, while other drugs should be avoided. Among the issues are accumulation of either the parent compound or its metabolites (resulting in hypoglycemia) or significant lactic acidosis. Conventional oral glycemic agents, such as sulfonylureas, present problems because of hypoglycemia. First-generation sulfonylureas (eg, chlorpropamide, tolazamide, and tolbutamide) generally should be avoided in patients with CKD because these agents rely on the kidney to eliminate both the parent drug and active metabolites, resulting in increased half-lives and risk of hypoglycemia.[5] Of the second-generation sulfonylureas available in the US (eg, glipizide, glyburide, glimepiride), glipizide is the preferred agent because it does not have active metabolites and does not increase the risk of hypoglycemia in patients with CKD.[5]
KDOQI guidelines on diabetes and CKD (2007) recommend that alpha-glucosidase inhibitors should generally be avoided in patients with advanced CKD and on dialysis (an update to these guidelines is expected to be published in the fall/winter of 2012). Metformin is a recommended first-line therapy in non-CKD secondary prevention and is not associated with an increased risk for hypoglycemia, but it can carry an increased risk of lactic acidosis in patients with moderate to advanced CKD. The FDA advises against metformin’s use in men with a serum creatinine of ≥ 1.5 mg/dL or women with a serum creatinine of ≥ 1.4 mg/dL. In the meglitinide class, nateglinide has increased active metabolites in patients with decreased kidney function.[86,87] Increased active metabolites do not occur with repaglinide, another meglitinide.[88] However, repaglinide can accumulate when the GFR ≤ 30 mL/min/1.73 m2.[88,89]
The thiazolidinediones pioglitazone and rosiglitazone do not lead to hypoglycemia and are metabolized by the liver. However, they can worsen fluid retention and should not be used in advanced heart failure and CKD. The FDA has restricted use of rosiglitazone based on information linking the medicine with increased cardiovascular events.[90] Healthcare providers and patients must be enrolled in the Avandia-Rosiglitazone Medicines Access Program in order to prescribe and receive rosiglitazone, which is no longer available through retail pharmacies.
A more recent development in the treatment of type 2 diabetes is the emergence of incretin hormone-based therapies, including glucagon-like peptide (GLP)-1 receptor agonists and dipeptidyl peptidase (DPP)-4 inhibitors. Generally, incretin-based therapies address various diabetes disease mechanisms, including beta-cell defects, hormone-related abnormalities, and accelerated gastric emptying.[91] Exenatide and liraglutide are injectable GLP-1 receptor agonists. The FDA recommends that exenatide should not be used in patients with advanced CKD or kidney failure.[92] Liraglutide is degraded elsewhere in the body, and the kidneys are not a major route of elimination. However, because of limited data on long term use, caution is advised in these patient populations. Therefore, the product labeling in the European Union advises that liraglutide currently cannot be recommended for use in moderate-to-severe kidney disease, including kidney failure.[93] DPP-4 inhibitors that are available in the US include sitagliptin, saxagliptin and linagliptin. Drugs within this class decrease the breakdown of the incretin hormones and improve both fasting and postprandial glucose levels.[94] All can be used in CKD patients but sitagliptin and saxagliptin may require dose adjustments in the presence of advanced CKD.
Insulin remains an effective alternative when oral therapy is insufficient, but it should also be adjusted based on frequent monitoring to balance the goals of glycemic control while avoiding hypoglycemia.[5] As with all medications, consult the package insert for full prescribing information, contraindications, and dose adjustments in the presence of specific comorbidities (eg, CKD).
The potential benefits of intensive glycemic control to reduce CVD events has been less clearly defined. A 10-year follow-up of the UK Prospective Diabetes Study (UKPDS) on type 2 diabetes showed that intensive control was found to reduce the overall microvascular complication rate by 25% compared with conventional treatment. Risk reductions in myocardial infarction and all cause death were also observed.[95] However, 3 randomized clinical trials [Action to Control Cardiovascular Risk in Diabetes (ACCORD), Action in Diabetes and Vascular Disease (ADVANCE), and Veterans Affairs Diabetes Trial (VADT)] did not show significant reduction in cardiovascular outcomes with intensive glycemic control.[96-98]
It has been suggested that an HbA1c target of < 7% may be appropriate for patients with short duration of diabetes, long life expectancy, and no significant cardiovascular disease. However, less stringent HbA1c goals may be appropriate for patients with a history of severe hypoglycemia, limited life expectancy, advanced microvascular or macrovascular complications, or extensive comorbid conditions.[78,79,99] Figure 10[79,99] outlines elements of decision-making that can be incorporated into glycemic management.
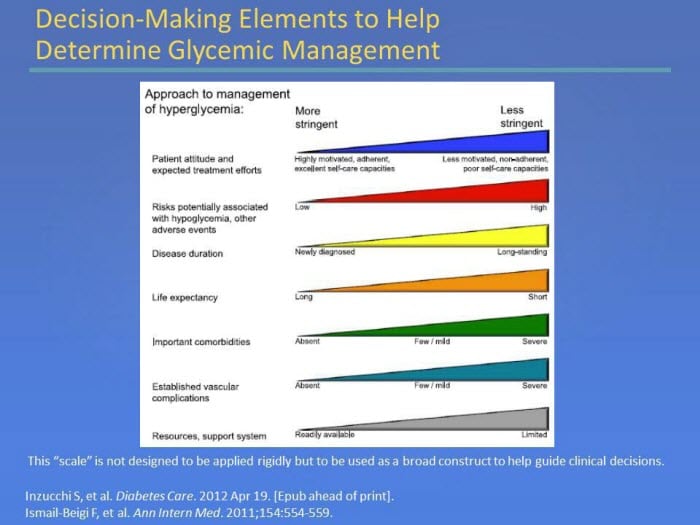
Figure 10. Decision-Making Elements to Help Determine Glycemic Management
Multidisciplinary and Multifactorial Approach
The overall objective of secondary CVD prevention is to reduce the risk of a major CVD event. To help meet this objective, patients should be counseled on therapeutic lifestyle changes (eg, smoking cessation, cardiac rehabilitation/physical activity, improved weight control). One comorbidity should not be treated in isolation, particularly in the case of CKD.[11,15] A multidisciplinary and multifactorial approach can also provide the best opportunity to slow the progression to kidney failure, reduce the risk of cardiovascular events, and improve outcomes.
Initial evaluation and re-evaluation of patients with CKD is extensive and may be performed over many visits with a variety of health-care providers working either alone or as part of a team. Healthcare providers are encouraged to set up a routine system for efficiently conducting these evaluations and referrals (Figures 11 and 12).[46]

Figure 11. Recommendations for Referral to Specialists* for Consultation and Co- Management of CKD
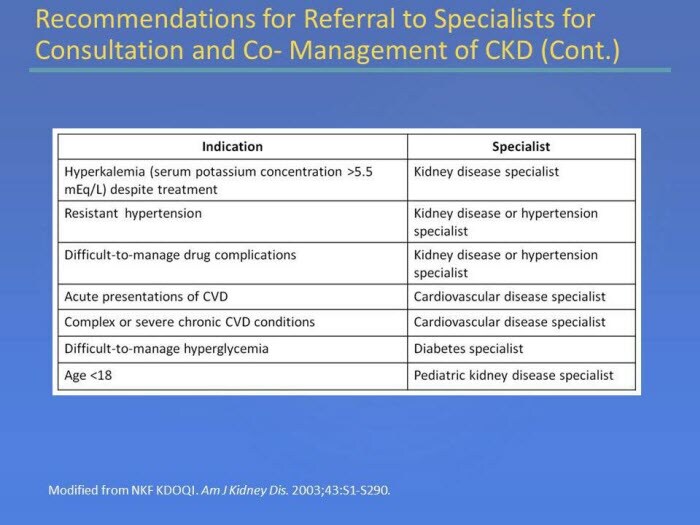
Figure 12. Recommendations for Referral to Specialists for Consultation and Co- Management of CKD (Cont.)
Because CKD is a CVD risk multiplier, strategies to monitor and manage kidney function should be an integral part of risk reduction. Patients with CKD also need special considerations when managing other comorbidities, such as hypertension and diabetes. Comprehensive risk factor management has been shown to benefit patients with multiple chronic diseases. A multidisciplinary team approach described by Bayliss et al involves shared care among an HMO-based nephrologist, pharmacy specialist, diabetes educator, dietitian, social worker, and nephrology nurse.[100] Both groups received usual primary care. In an integrated care setting, the care from a multidisciplinary team resulted in a slower decline in glomerular filtration rate (GFR) than usual care. In multivariate repeated-measures analyses, multidisciplinary therapy was associated with a mean annual decline in GFR of 1.2 vs 2.5 mL/min/1.73 m2 for usual care (Figure 13).[100]
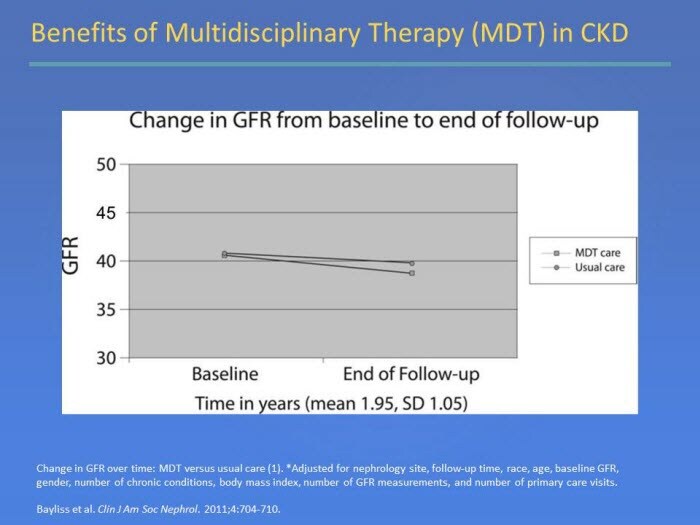
Figure 13. Benefits of Multidisciplinary Therapy (MDT) in CKD
A retrospective, case-control study demonstrated that patients attending a multidisciplinary clinic are better prepared for dialysis treatment, have fewer hospital admissions after start of dialysis, and have a higher patient survival compared to those attending a traditional nephrology clinic.[101]
In at-risk patients with type 2 diabetes, intervention with multiple drug combinations and behavior modification has shown sustained beneficial effects with respect to vascular complications and on rates of death from any cause and from cardiovascular causes. The Steno-2 Study compared the effect of a targeted, multifactorial intervention on modifiable risk factors for cardiovascular disease in patients with type 2 diabetes and microalbuminuria.[102] The primary end point of this open, parallel trial was a composite of death from cardiovascular causes, nonfatal myocardial infarction, nonfatal stroke, revascularization, and amputation. The authors concluded that a target-driven, long-term intervention aimed at multiple risk factors in patients with type 2 diabetes and microalbuminuria reduces the risk of cardiovascular and microvascular events.
Lifestyle Changes
Guidelines emphasize numerous lifestyle modifications in secondary prevention of CVD, including programs for smoking cessation, physical activity, cardiac rehabilitation, and weight management.[1,5,11,21,46] Cigarette smoking is clearly associated with the risk of CVD as well as progression of CKD.
In the case of secondary prevention of CVD, cardiac rehabilitation and physical activity are very important secondary prevention strategies. Individuals who are physically active are less likely to develop chronic diseases such as diabetes, hypertension, CKD and CVD than their sedentary counterparts.[21,46,103,104] Therapeutic lifestyle changes (TLC) should include diet, weight reduction if needed, and increased physical activity for the promotion of cardiovascular health and prevention of dyslipidemia and other risk factors for CVD (Figure 14).[46]
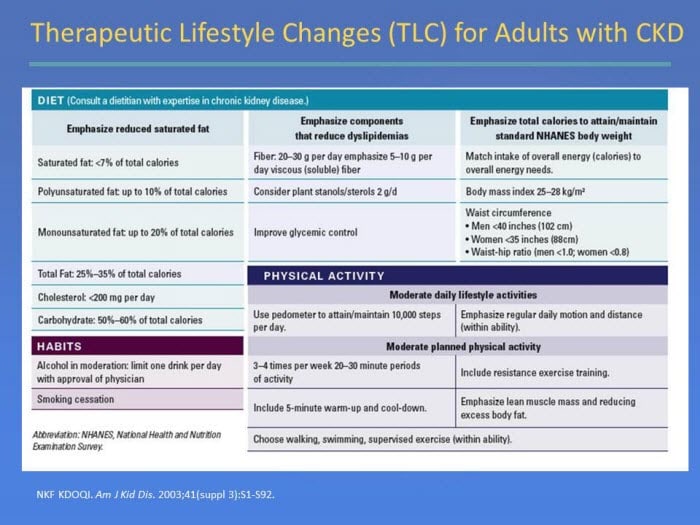
Figure 14. Therapeutic Lifestyle Changes (TLC) for Adults with CKD
SUMMARY
Secondary prevention of CVD remains a complex challenge. Special considerations for comorbidities like CKD and diabetes need to be factored into the patient’s care. This may include the use of ACE inhibitors/ARBs (not only for BP control, but also for renoprotection), dose adjustments, and avoiding the use of certain medications contraindicated in patients with CKD. Prevention strategies that include long-term, multidisciplinary, and multifactorial interventions can offer the best opportunity to improve outcomes.
Comments
Post a Comment