INTRODUCTION
Human epidermal growth factor receptor 2 (HER2) is overexpressed on the cell surface and/or there is gene amplification in approximately 20% of all breast cancers.[1] As a result, approximately 45,000-46,000 American women develop HER2-positive breast cancer each year.[2,3] HER2 status has prognostic significance: HER2-positive tumors are more aggressive and, without specific therapy, are associated with worse outcomes.[4] However, in 2012 the most important role of HER2 is determination of eligibility for HER2-targeted therapy with trastuzumab or lapatinib.[1,5]
Although HER2-targeted therapy has improved outcomes in early breast cancer and in the metastatic setting, in the latter case it is typical to see progression after an initial response.[6,7] Therefore, research continues into optimizing the use of currently available agents and into novel agents including the novel HER2 antibody pertuzumab, the conjugate trastuzumab emtansine, and novel tyrosine kinase inhibitors such as afatinib and neratinib.
This monograph reviews the rationale for these new approaches and novel agents—including the antibody pertuzumab, recently approved by the US Food and Drug Administration (FDA)—and the clinical data to date.
HER2 SIGNALING AND CROSSTALK
HER2 is a member of the HER family of tyrosine kinase cell surface receptors, also called ErbB. They are named HER1/ErbB1 (or epidermal growth factor receptor [EGFR]), HER2/ErbB2, HER3/ErbB3, and HER4/ErbB4.[8] A number of ligands have been identified that bind to HER1, HER3, and HER4, including EGF, transforming growth factor alpha (TGF-α), and the "regulins" such as amphiregulin, epiregulin, and neuregulin-1.[8,9] Binding of the ligand to the cell surface receptor induces conformational changes to that receptor, and dimers are formed. This in turn activates the associated tyrosine kinase and, depending on the receptor, downstream signaling pathways such as the Ras-Raf-MAPK (mitogen-associated protein kinase) pathway, phosphoinositide 3-kinase (PI3K)-AKT pathway, and protein kinase C (PKC) (Figure 1).[9]
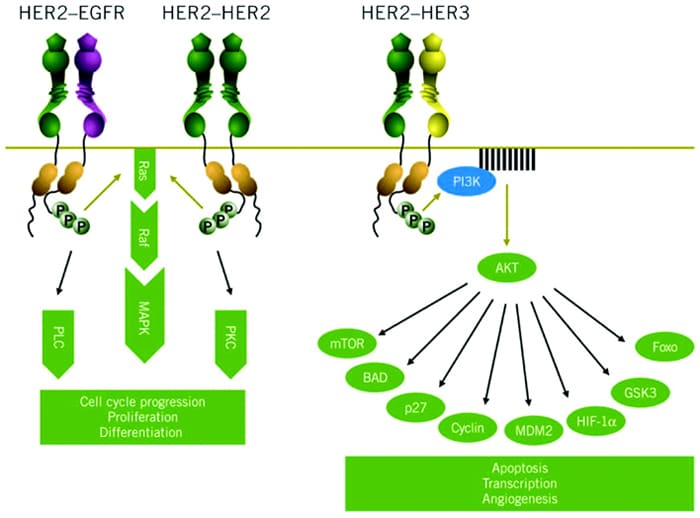
Figure 1. Signaling pathways activated by HER2.[9]
HER2 is unusual among the HER family in that it has no known ligands. Instead, HER2 is the preferred dimerization partner for other members of the family and appears to act as a coreceptor to improve ligand binding and signal transduction.[10] As such, HER2 can form heterodimers with other members of the HER family and can also form homodimers (ie, HER2/HER2 dimers; see Figure 1).[9]
HER2-mediated signaling is associated with cell proliferation, survival, and motility.[11] In HER2-postive cells these growth signals are thought to be driven mainly through HER2/HER3 heterodimers. Because HER3 lacks an associated tyrosine kinase, it requires HER2 for signal transduction, which results in activation of the PI3K-AKT pathway (Figure 1).[9,12] HER2 homodimers activate the Ras-Raf pathway, and it has been shown that the monoclonal antibody trastuzumab preferentially inhibits these HER2 homodimers, which has implications for both efficacy and resistance.[13]
ESTABLISHED HER2-TARGETED THERAPY
Two HER2-targeted therapies are currently available for the management of breast cancer: the immunoglobulin G1 (IgG1) antibody trastuzumab and the tyrosine kinase inhibitor lapatinib.[7,11] Trastuzumab binds to the extracellular HER2 receptor, where it disrupts HER2 signaling, downregulates HER2 expression, inhibits cell cycle progression, and induces antibody-dependent cell-mediated cytotoxicity (ADCC).[14,15] In addition, trastuzumab inhibits HER2 shedding,[16] which reduces levels of p95-HER2.[15] Lapatinib is a small-molecule inhibitor of the tyrosine kinase associated with HER2. It prevents phosphorylation and thereby inhibits downstream signaling. Lapatinib also inhibits the tyrosine kinase associated with HER1 (EGFR).[17]
Trastuzumab is FDA-approved for use in the adjuvant setting and also in patients with advanced/metastatic breast cancer.[18]It is also FDA-approved for gastric cancer,[18] which will not be discussed in detail within this activity. Lapatinib is FDA-approved for patients with advanced/metastatic breast cancer.[19]
Adjuvant use of trastuzumab in combination with cytotoxic chemotherapy is recommended for patients with HER2-positive, node-positive disease, based on the results from 5 pivotal studies.[5] These trials are summarized in Figure 2 and illustrate significant benefits in terms of progression-free survival (PFS) and, in some trials, overall survival (OS).[20-25] Although the FinHer trial utilized just 9 weeks of trastuzumab,[24] based on the results of the other 4 studies 1 year of adjuvant trastuzumab is the recommended duration.[5]
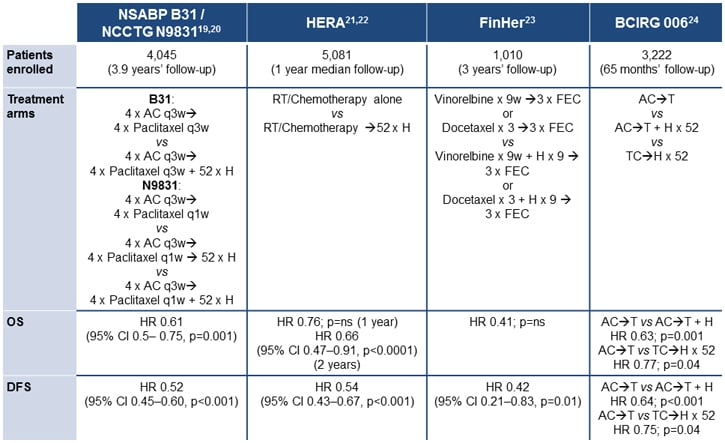
Figure 2. Adjuvant trastuzumab: selected studies.[20-25]
The TEACH (Tykerb Evaluation After Chemotherapy) study assessed the effect of delayed lapatinib in patients with HER2-positive breast cancer who had completed adjuvant chemotherapy but not received trastuzumab (eg, due to completion of chemotherapy before trastuzumab was available).[26] Patients had a median time between diagnosis and study entry of 2.7 years, and after 4 years' follow-up, no benefit in terms of PFS was detected (hazard ratio [HR], 0.83; 95% confidence interval [CI], 0.70-1.00; P = .053). However, in a preplanned subgroup analysis, significant benefit from lapatinib was observed in patients with hormone-receptor-negative disease (HR, 0.68; 95% CI, 0.52-0.89) and in those randomized within 1 year of diagnosis (HR, 0.70; 95% CI, 0.50-0.99), particularly in those individuals with tumors that were confirmed HER2-positive by central review.[26,27] The ALTTO (Adjuvant Lapatinib and/or Trastuzumab Treatment Optimisation) study is an ongoing trial, originally of 4 arms, comparing lapatinib alone, trastuzumab alone, the sequence (trastuzumab for 12 weeks followed by lapatinib), and the combination, as adjuvant therapy after chemotherapy.[11,28] More than 8000 patients have been enrolled; however, an interim analysis has indicated that the lapatinib-alone arm is not likely to meet the prespecified endpoint of noninferiority to trastuzumab alone, and this arm has been discontinued.
In addition, both trastuzumab and lapatinib are recommended in patients with advanced or metastatic HER2-positive breast cancer, with lapatinib recommended by the National Comprehensive Cancer Network (NCCN) for patients who progress after trastuzumab therapy.[5] Studies have demonstrated benefits from trastuzumab as monotherapy[29]; however, it is more usual to use trastuzumab in combination with cytotoxic chemotherapy.[5] A number of agents are recommended as suitable for use with trastuzumab, including paclitaxel, paclitaxel with carboplatin, docetaxel, vinorelbine, and capecitabine (results from selected studies are shown in Figure 3).[30-34]
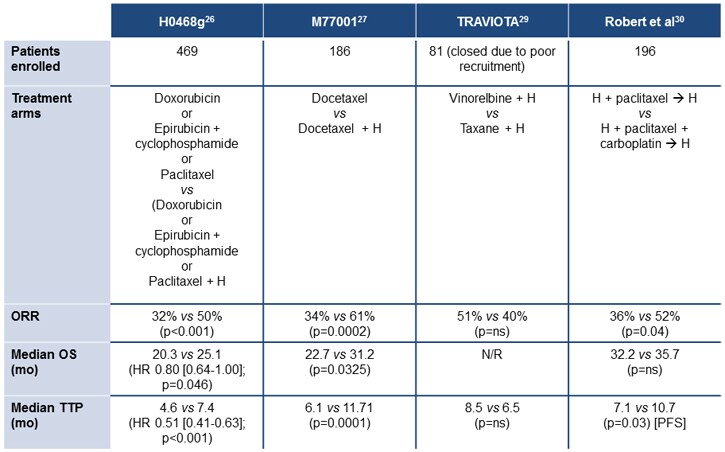
Figure 3. Trastuzumab in advanced/metastatic breast cancer.[30,31,33,34]
At the 2012 annual meeting of the American Society of Clinical Oncology (ASCO®), results were reported from the National Cancer Institute of Canada Clinical Trials Group's NCIC CTG MA.31 study, which compared first-line trastuzumab and lapatinib in patients with metastatic breast cancer. A total of 652 patients were enrolled, with data from 636 available (including 525 with HER2 status confirmed by central laboratory). Randomization was to taxane therapy (weekly paclitaxel or docetaxel) for 24 weeks in combination with either lapatinib or trastuzumab, followed by HER2-targeted therapy until progression.[35]After a median 13.6 months' follow-up, lapatinib was associated with inferior PFS compared with trastuzumab (8.8 months vs 11.4 months; HR, 1.33; 95% CI, 1.06-1.67; P = .01).
A phase 2 study of lapatinib in patients with previously treated metastatic or advanced breast cancer evaluated the HER2-positive cohort, all of whom had received trastuzumab, and reported objective responses in 4.3% of patients, with a median PFS of 9.1 weeks.[36] In contrast, there was no detectable benefit from lapatinib in HER2-negative patients, despite the activity of this compound against HER1. Following this and other phase 2 trials, the pivotal study compared capecitabine monotherapy with the combination of capecitabine and lapatinib in patients with trastuzumab-refractory advanced/metastatic disease.[37] This study reported significant benefits from the addition of lapatinib in terms of PFS (HR, 0.49; 95% CI, 0.34-0.71; P < .001), with a median time to progression of 8.4 months vs 4.4 months. Overall responses were reported in 22% of patients receiving lapatinib plus capecitabine, compared with 14% of those given capecitabine alone (P = not significant).
Benefits have also been reported for the addition of lapatinib to trastuzumab vs lapatinib alone in a chemotherapy-free regimen in patients with heavily pretreated metastatic breast cancer (Figure 4), indicating the benefits from "dual blockade" of the HER2 receptor.[38]
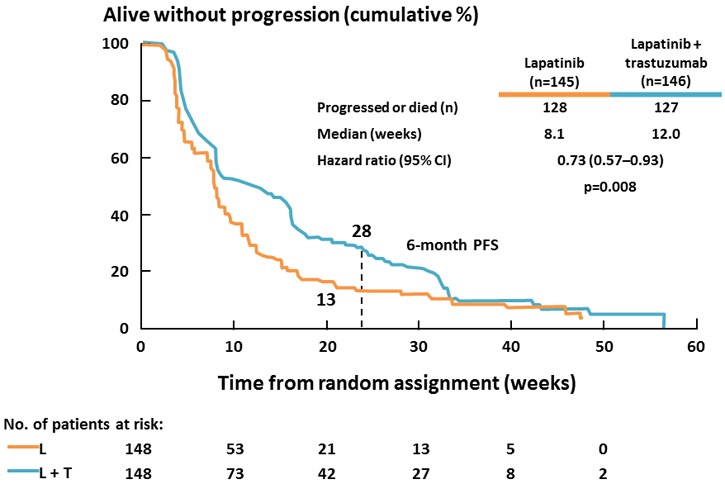
Figure 4. The combination of lapatinib and trastuzumab vs lapatinib alone in patients with trastuzumab-refractory metastatic breast cancer.[38]
Although not FDA-approved, studies have also assessed the effect of neoadjuvant trastuzumab added to paclitaxel-FEC (fluorouracil, epirubicin, and cyclophosphamide)[39] and to doxorubicin, paclitaxel, cyclophosphamide, methotrexate, and fluorouracil (the NOAH, or Neoadjuvant Herceptin, trial).[40] The GeparQuinto (GBG44) trial compared the addition of trastuzumab or lapatinib to neoadjuvant chemotherapy with epirubicin and cyclophosphamide followed by docetaxel (EC-T). Pathologic complete responses were reported significantly more frequently in the trastuzumab (EC-TH) group (93/307 evaluable; 30%) compared with the lapatinib (EC-TL) group (70/308; 23%) (P = .04). Although there was more edema and dyspnea in the EC-TH group, there was more diarrhea and skin rash in the EC-TL group, and more patients discontinued in the EC-TL arm (33% vs 14%).[41] The CHER-LOB (Chemotherapy, Herceptin and Lapatinib in Operable Breast Cancer ) study randomized 121 patients to paclitaxel for 12 weeks followed by 4 courses of FEC with lapatinib, trastuzumab, or the combination. Pathologic complete responses were seen significantly more frequently with the combination of trastuzumab and lapatinib (46.7%) than with either agent alone (25% and 26.3%; P = .019).[42] More recently, the combination of lapatinib and trastuzumab was also found to be more effective than either agent alone when added to neoadjuvant doxorubicin and cyclophosphamide followed by weekly paclitaxel (AC-T) chemotherapy, with pathologic complete responses in 62% of patients, compared with 52.5% for AC-T-trastuzumab and 53.2% for AC-T-lapatinib (P = .075).[43]
The phase 3 NeoALTTO (Neoadjuvant Lapatinib and/or Trastuzumab Treatment Optimisation) trial was a comparison of lapatinib, trastuzumab, and the combination for 6 weeks followed by a further 12 weeks of weekly paclitaxel before surgery in 455 patients with treatment-naïve, operable breast cancers greater than 2 cm in diameter. Adjuvant chemotherapy was combined with the same HER2-targeted therapy used prior to surgery.[44] This study also reported significantly more pathologic complete responses with the combined HER2 blockade, with no difference between the 2 single-agent HER2-targeted therapy arms (Figure 5). Grade 3 diarrhea was more common in lapatinib-treated patients (23% for monotherapy, 21% for the combination) than with trastuzumab (2%), and grade 3 liver enzyme abnormalities also occurred more frequently with lapatinib (17.5%) and lapatinib/trastuzumab (9.9%) than with trastuzumab (7.4%).[44]
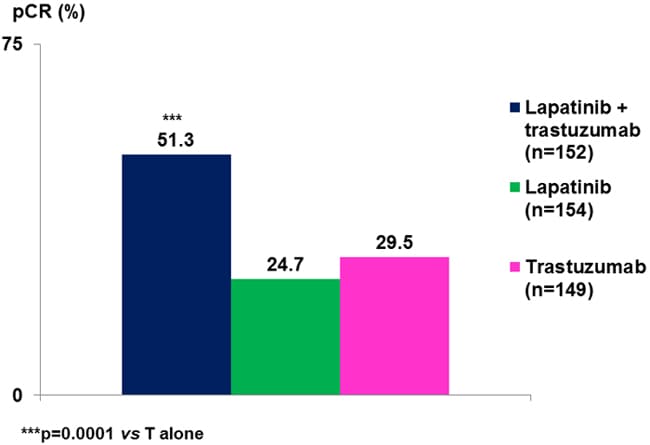
Figure 5. NeoALTTO: pathologic complete response rate increased with dual HER2 blockade.[44]
RESISTANCE MECHANISMS: HER2-TARGETED AGENTS
Despite the clinical benefits reported with HER2-targeted therapy, both de novo and acquired resistance to trastuzumab and lapatinib has been reported.[15] In patients with metastatic breast cancer, loss of response to HER2-targeted therapy is the norm.
The effect of lapatinib in patients with trastuzumab-refractory disease and the relative benefits of dual inhibition with lapatinib and trastuzumab in this setting provide some insights into the potential mechanisms of this resistance. This is complemented by preclinical and laboratory analysis of downstream signaling pathways, which has confirmed that multiple mechanisms of resistance exist. These can be classified as barriers to trastuzumab binding, upregulation of downstream signaling, crosstalk, and failure to trigger ADCC (Figure 6).[15,45] The majority of these mechanisms also allow tumor cells to escape lapatinib, although activation of alternate tyrosine kinases is also an important mechanism.[46] Mutations in the HER2 gene appear to be rare, however,[47] unlike acquired resistance to HER1/EGFR tyrosine kinase inhibitors.
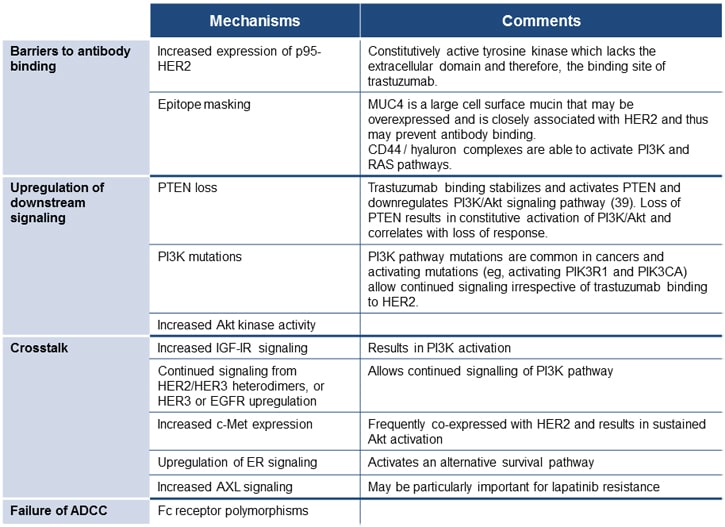
Figure 6. Mechanisms of resistance to HER2-targeted therapy.[15,45-47]
These findings have prompted research not only into alternative uses of the existing HER2-targeted therapy, but also into the combined use of trastuzumab and lapatinib to provide a more complete blockade of signaling. Dual blockade of HER2 by the combination of lapatinib and trastuzumab may, however, result in upregulation of the estrogen receptor, allowing it to function as an alternative survival pathway.[48] Therefore, novel agents that circumvent some of these mechanisms are also being actively studied. The most advanced of these agents are described in the next section.
NOVEL THERAPEUTICS: MECHANISMS AND CLINICAL DATA
Pertuzumab
Because of the importance of dimerization in the HER2 signaling cascade, a rational approach is to inhibit the dimerization of HER2, either as homo- or heterodimers. Pertuzumab is the first-in-class "HER dimerization inhibitor"[49],for which several key pieces of evidence became available in 2012, and is now FDA-approved for use with trastuzumab and chemotherapy for treatment-naïve, HER2-positive, metastatic breast cancer.[50]
Pertuzumab binds to the dimerization domain of HER2, a different epitope than the binding site for trastuzumab, where it prevents HER2 forming dimers with ligand-activated members of the HER/ErbB family (HER1, HER3, and HER4).[49,51]
Although preclinical data suggested that pertuzumab might have an antitumor effect in the absence of HER2 overexpression, a clinical trial in HER2-negative breast cancer found limited efficacy, with generally stable disease of short duration.[52]However, synergism was reported in vitro and in animal models of HER2-positive breast cancer; in these models pertuzumab was found to activate ADCC.[51,53]
A phase 2 study (BO17929) in patients with advanced/metastatic breast cancer that had progressed after trastuzumab therapy evaluated administration of pertuzumab every 3 weeks with trastuzumab weekly or every 3 weeks. It reported an objective response rate of 24%, including 5 of 66 patients (7.6%) who achieved a complete response. A median PFS of 5.5 months was reported, and tolerability was acceptable, with minimal cardiac dysfunction and no withdrawals due to cardiac toxicity.[54] A third cohort of patients was subsequently recruited and given pertuzumab monotherapy. All 29 patients in this cohort experienced progression, with an objective response rate of 3.4% and a PFS of 7 weeks. A proportion of these patients subsequently received the combination of pertuzumab plus trastuzumab, resulting in an objective response rate of 17.6% (3 patients) and an extended PFS of 17.4 weeks.[55] These observations confirmed that the combination of pertuzumab and trastuzumab is more efficacious than pertuzumab alone and has activity in patients who progress on trastuzumab, implying that this combination is able to at least partially overcome trastuzumab resistance.
Following early trials, the CLEOPATRA (Clinical Evaluation of Pertuzumab and Trastuzumab) study recruited 808 patients with HER2-positive, metastatic breast cancer who had received no therapy for their metastatic disease other than 1 hormonal treatment.[56] Adjuvant or neoadjuvant trastuzumab was allowed if there was an interval of at least 12 months posttherapy.
Patients were assigned to either docetaxel every 3 weeks with trastuzumab or the same combination with pertuzumab (Figure 7). The primary endpoint was PFS, with an 80% power to detect a 33% improvement in the pertuzumab group. Secondary endpoints included OS, objective response rate, and safety (Figure 7).
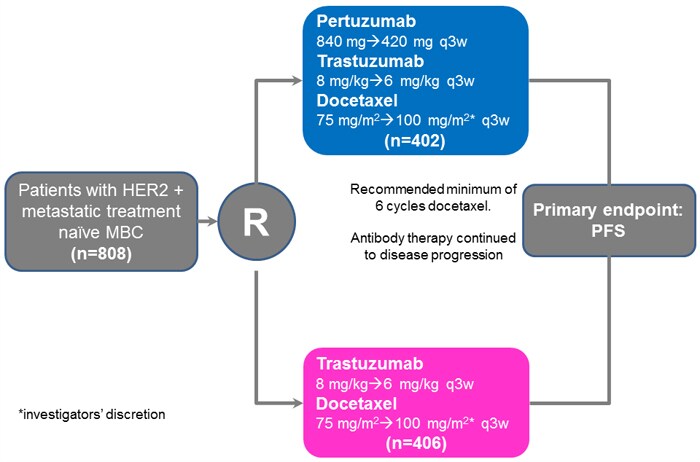
Figure 7. Design of CLEOPATRA: pertuzumab in combination with trastuzumab and docetaxel.[56]
Randomized patients had a median age of 54 years and were largely white (59%) or Asian (32%), with an ECOG Performance Status of 0 (65%) or 1 (35%), a HER2 status by immunohistochemistry (IHC) of 3+ (89%), and positive by fluorescence in situ hybridization (FISH) (95%). Approximately half of the patients had received adjuvant therapy, but only 11% had received prior trastuzumab in this setting.
The median PFS was prolonged by 6.1 months by pertuzumab (Figure 8), giving an HR for death or progression of 0.62 (95% CI, 0.51-0.75; P < .001), an observation repeated in all predefined subgroups (prior adjuvant therapy, age, geographic region, race, visceral vs nonvisceral disease, hormone receptor status, etc).[56]
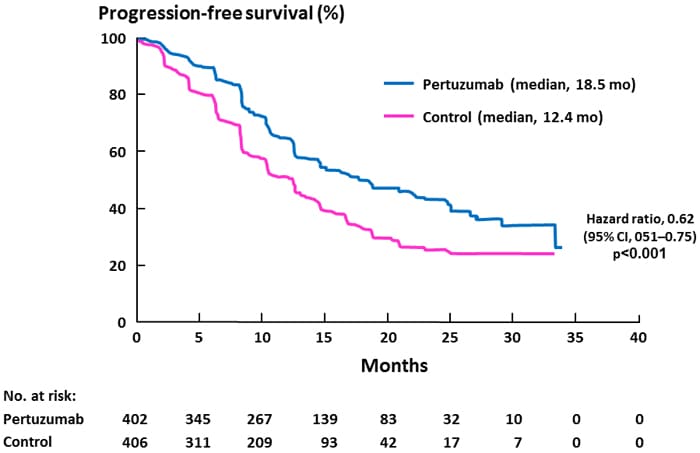
Figure 8. PFS in CLEOPATRA: pertuzumab in combination with trastuzumab and docetaxel.[56]
An interim analysis of OS after 165 events did not meet prespecified criteria for significance, but showed a strong trend for superiority with pertuzumab (69 events vs 96 events; 17.2% vs 23.6%; HR, 0.64; 95% CI, 0.47-0.88; P = .005). Final analysis will be undertaken after 385 deaths; current follow-up is 19.3 months. Objective response rates also indicated a strong trend for benefit with pertuzumab (80.2% vs 69.3%; P = .001); final confirmation of this exploratory analysis will be undertaken after the final analysis for OS.[56]
Adverse events were similar across the 2 treatment arms; in the pertuzumab combination cohort, diarrhea, rash, mucosal inflammation, febrile neutropenia, and dry skin were 5% or more frequently reported; constipation, peripheral edema, and asthenia were at least 5% less common (Figure 9).[56]
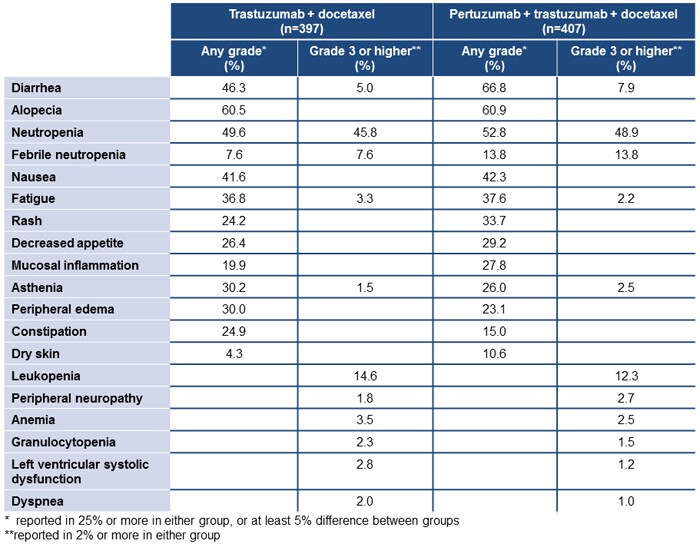
Figure 9. Adverse events in CLEOPATRA: pertuzumab in combination with trastuzumab and docetaxel.[56]
Left ventricular systolic dysfunction was more common in pertuzumab-treated patients (8.3% vs 4.4%), although grade 3 or higher events were more common in the control arm (2.8% vs 1.2%).[56]
Discontinuation due to adverse events was most commonly of docetaxel (23% of patients in each arm) compared with all therapy (5.3% for trastuzumab/docetaxel and 6.1% for pertuzumab/trastuzumab/docetaxel). This was associated with a reduction in grade 3 events, although diarrhea of grade 3 or higher remained more common in the pertuzumab/trastuzumab-treated patients.[57] In addition, the triple therapy regimen was not associated with a decrease in quality of life using the FACT-B questionnaire, and there was a delay in deterioration on the breast cancer symptom scale.[58]
Based on these data, pertuzumab is FDA-approved for use with trastuzumab and chemotherapy in patients with metastatic HER2-positive breast cancer.[50] Ongoing studies of pertuzumab include the PHEREXA (Pertuzumab HERceptin Evaluation with XelodA)] study, assessing the combination of trastuzumab and capecitabine with or without pertuzumab as a second-line therapy for metastatic breast cancer; and PERUSE, a single-arm study of first-line pertuzumab with trastuzumab and a taxane in metastatic breast cancer.[59,60] The MARIANNE trial will assess the combination of pertuzumab and the conjugate trastuzumab emtansine (Figure 10).[61]
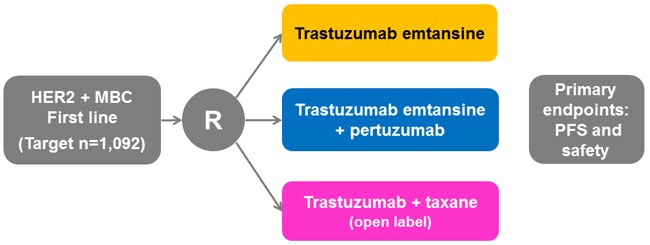
Figure 10. Design of MARIANNE: pertuzumab with trastuzumab emtansine in metastatic breast cancer.[61]
In addition, the activity of pertuzumab in earlier breast cancer is being actively researched. The NeoSphere trial was an open-label phase 2 study comparing 4 neoadjuvant cycles of trastuzumab plus docetaxel, pertuzumab plus trastuzumab plus docetaxel, pertuzumab plus trastuzumab, and pertuzumab plus docetaxel.[62] A total of 417 patients were randomized and the primary endpoint was pathologic complete response.
The triple combination was found to produce significantly more pathologic complete responses (Figure 11), with serious adverse events being similar in all arms containing docetaxel but less frequent in the pertuzumab/trastuzumab arm. The most frequently reported grade 3 or higher events were neutropenia, febrile neutropenia, and leukopenia.[62]
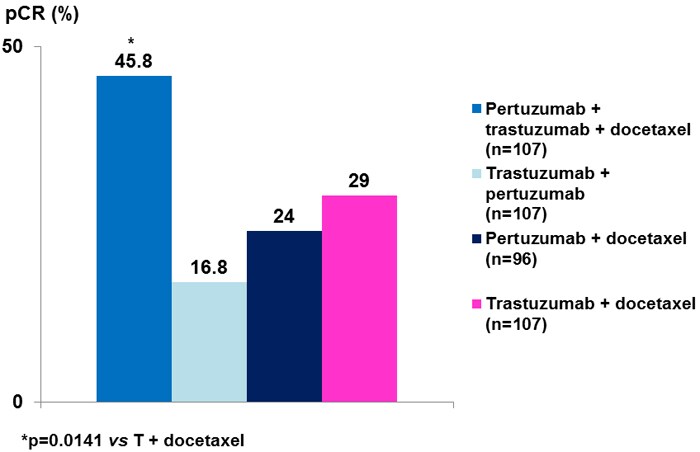
Figure 11. Pathologic complete responses in NeoSphere: neoadjuvant pertuzumab and trastuzumab.[62]
The TRYPHAENA (Trastuzumab plus Pertuzumab in Neoadjuvant HER2-Positive Breast Cancer) trial is currently evaluating the tolerability of neoadjuvant pertuzumab with trastuzumab administered either concurrently or sequentially with FEC or concurrently with an anthracycline-free regimen (docetaxel plus carboplatin).[51,63] In addition, the APHINITY (Pertuzumab and Herceptin IN IniTial TherapY of Breast Cancer) trial is assessing the efficacy and tolerability of adjuvant pertuzumab given with trastuzumab and chemotherapy.[51,64]
Trastuzumab Emtansine (Trastuzumab-DM1)
Trastuzumab emtansine, formally termed trastuzumab-DM1, is a novel drug-antibody conjugate in development for breast cancer.[65] The mechanism of action uses the binding of trastuzumab to HER2 to inhibit HER2-overexpressing cells, as discussed earlier. However, in addition, a cytotoxic agent (DM1) remains attached to the extracellular surface receptor until endocytosis transports the HER2 receptor/trastuzumab/DM1 complex into the cytoplasm.[65,66] It is thought that once the drug is inside the cell, lysis results in free DM1, which can then exert antineoplastic effects through its effects on tubulin.[66]This targeted delivery of DM1 within the cytoplasm results in lower exposure of nontumor cells to DM1 while enhancing the effects of trastuzumab.[66]
Single-arm studies have confirmed the therapeutic effect of trastuzumab emtansine in patients with HER2-positive breast cancer (Figure 12).[67,68]
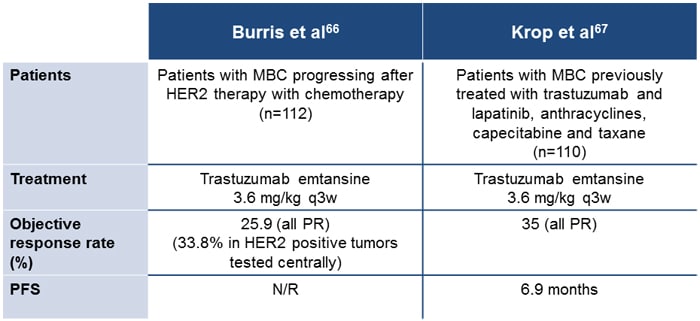
Figure 12. Single-arm phase 2 trials of trastuzumab emtansine.[67,68]
At the 2011 meeting of the European Society for Medical Oncology (ESMO), final results were reported from a randomized phase 2 trial of trastuzumab emtansine 3.6 mg/kg every 3 weeks compared with trastuzumab plus docetaxel every 3 weeks.[69] This study enrolled 137 patients with previously untreated HER2-positive, metastatic breast cancer. Although objective response rates were similar (64% for trastuzumab emtansine vs 58% for trastuzumab/docetaxel), trastuzumab emtansine was associated with significantly prolonged PFS (Figure 13).
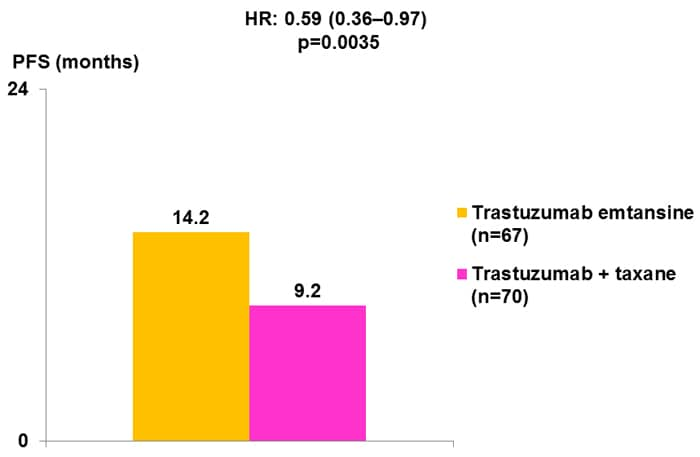
Figure 13. Results from a randomized phase 2 trial of trastuzumab emtansine.[69]
In addition, with a median duration of follow-up of approximately 14 months in each arm, tolerability was improved with trastuzumab emtansine compared with trastuzumab and docetaxel. Grade 3 or 4 events were less common (46.4% vs 89.4%), as were serious events (18.8% vs 25.8%); as a result, there were fewer discontinuations due to adverse events (7.2% vs 28.8%), and at the data cutoff 43.3% of patients were continuing trastuzumab emtansine (compared with 21.4% who were continuing trastuzumab/docetaxel). The adverse event profiles were different; trastuzumab emtansine was associated with fatigue, nausea, pyrexia, and increased aspartate aminotransferase (AST) levels, while trastuzumab/docetaxel was associated with alopecia, neutropenia, diarrhea, and fatigue.[69]
Preliminary results from the phase 3 EMILIA (Trastuzumab Emtansine vs Capecitabine and Lapatinib in Patients With HER2-Positive Locally Advanced or Metastatic Breast Cancer) study of trastuzumab emtansine compared with capecitabine plus lapatinib in patients progressing after trastuzumab and a taxane (Figure 14) were also recently presented at ASCO®.[70]
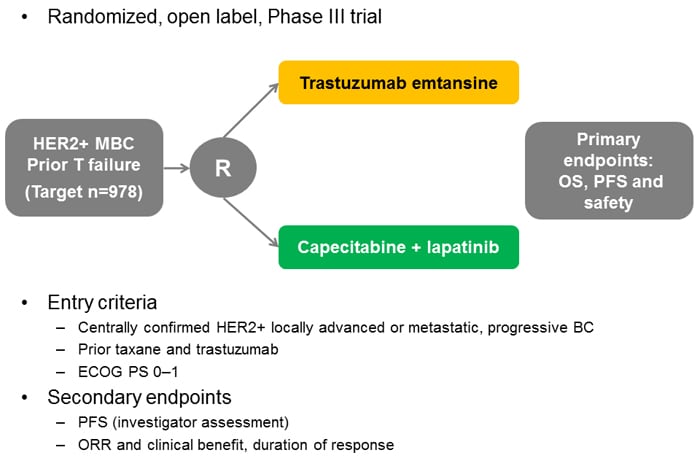
Figure 14. Design of the EMILIA study: trastuzumab emtansine or lapatinib plus capecitabine in patients progressing after trastuzumab.[70]
The primary endpoints were PFS, OS, and safety. At the time of reporting, median follow-up was 12.4 and 12.9 months for the lapatinib and trastuzumab emtansine arms, respectively. PFS and OS were significantly prolonged by trastuzumab emtansine (Figure 15); 2-year OS was estimated as 65.4% (trastuzumab emtansine) vs 47.5% (lapatinib plus capecitabine).[70]
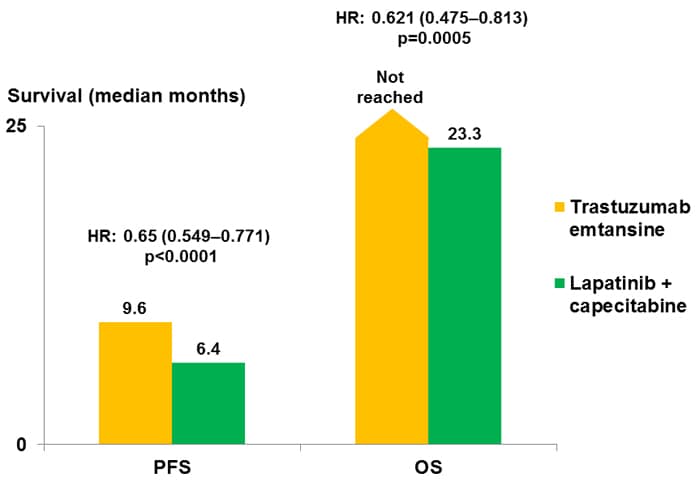
Figure 15. Results of the EMILIA study: trastuzumab emtansine or lapatinib plus capecitabine in patients progressing after trastuzumab.[70]
The most common grade 3 or higher adverse events with trastuzumab emtansine were thrombocytopenia (a rate of 12.9%, vs 0.2% in the lapatinib/capecitabine arm), increased AST levels (4.3% vs 0.8%), and increased alanine aminotransferase (ALT) levels (2.9% vs 1.4%), and for lapatinib plus capecitabine, diarrhea (a rate of 20.7%, vs 1.6% in the trastuzumab emtansine arm), hand-foot syndrome (16.4% vs 0), and vomiting (4.5% vs 0.8%).[70]
Clinical trials ongoing with trastuzumab emtansine include TH3RESA, which is comparing trastuzumab emtansine with clinicians' choice after failure of 2 prior HER2-targeted regimens,[71] and MARIANNE (Figure 10).
Novel Tyrosine Kinase Inhibitors
Several tyrosine kinase inhibitors that are under development aim to improve on the pharmacodynamic properties of lapatinib. Two of these that have shown promise in breast cancer are afatinib and neratinib; both are "irreversible" inhibitors of the HER2 and HER1 tyrosine kinase.[72] Unlike lapatinib, these agents form a covalent bond that is irreversible. Therefore, receptor signaling is inhibited until new receptor/tyrosine kinase complexes are synthesized.
A phase 2 study of afatinib has been reported in patients with advanced/metastatic HER2-positive breast cancer that had progressed after trastuzumab or who were intolerant of trastuzumab therapy.[73] A total of 41 patients received therapy with afatinib; most had received 3 prior lines of chemotherapy and 68% had received more than 1 year of trastuzumab. A partial response to monotherapy was reported in 4 patients (10%); median PFS was 15 weeks and median OS was 61 weeks. Treatment was associated with grade 3 or 4 diarrhea and rash.
Studies of afatinib in breast cancer are currently enrolling patients and include a phase 2 study of afatinib with or without vinorelbine in HER2-positive inflammatory breast cancer[74] and the Lux-Breast trials (Figure 16).[75-77] Phase 1/2 studies of neratinib have also reported effects in patients with HER2-positive breast cancer, although to date, no phase 2 clinical results have been presented or published.[9]
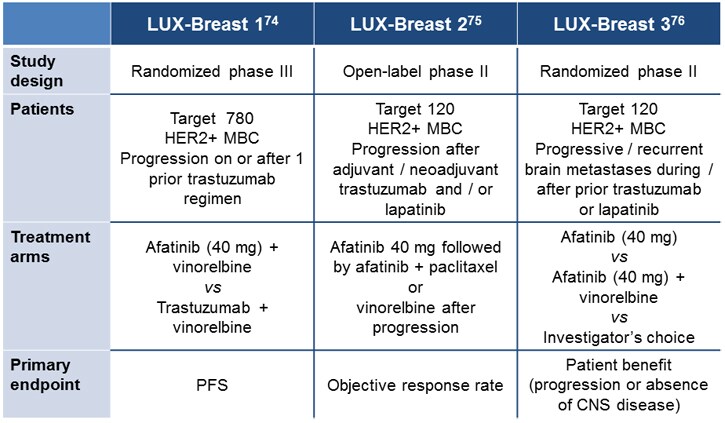
Figure 16. Ongoing LUX-Breast clinical trials with afatinib in breast cancer.[75-77]
SUMMARY
HER2-targeted therapy has made a substantial difference to the 45,000 American women who develop HER2-positive breast cancer annually. Two agents are established for the treatment of HER2-positive breast cancer: the antibody trastuzumab and the HER1/HER2 tyrosine kinase inhibitor lapatinib. Although effective, treatment with HER2-targeted therapy is associated with loss of response, at least in the advanced/metastatic setting. Mechanisms of resistance to HER2-targeted agents include "escape" by activation of alternative signaling pathways, one of the most important being the formation of HER2 heterodimers. Recent evidence from studies of trastuzumab combined with lapatinib in the advanced/metastatic and neoadjuvant settings provides proof of concept that more complete inhibition of HER2 can improve clinical efficacy.
The novel HER2 antibody pertuzumab inhibits the formation of HER2 dimers and thus has activity in patients losing response to trastuzumab and as first-line therapy. The CLEOPATRA study reported that the combination of pertuzumab and trastuzumab was more effective than trastuzumab when added to cytotoxic chemotherapy in terms of PFS, with strong trends for improved OS and response rate in treatment-naïve, metastatic, HER2-positive breast cancer. Pertuzumab is now FDA-approved for this indication, while studies are further evaluating its use in treatment-experienced and treatment-naïve patients.
Other novel HER2-targeted agents in development include the novel conjugate trastuzumab emtansine. The phase 3 EMILIA study recently reported that this agent significantly prolonged PFS and OS compared with lapatinib plus capecitabine in patients with advanced HER2-positive breast cancer whose disease was progressing after treatment with a taxane plus trastuzumab. In addition, therapy with trastuzumab emtansine was better tolerated.
Novel tyrosine kinase inhibitors of the HER2 receptor that may represent an advance over existing agents are also in development. For example, afatinib and neratinib are irreversible HER2/HER1 inhibitors that have shown clinical effects in early clinical trials in breast cancer.
As pertuzumab enters routine clinical practice, and other novel agents also near clinical reality, it will be necessary to reevaluate established treatment paradigms for HER2-positive breast cancer to make optimal use of these advances and thereby improve patient outcomes.
Comments
Post a Comment